Blog
Understanding drug test cutoffs for procurement decisions

TL;DR:
- Procurement officers must ensure drug test cutoff values are calibrated to current federal standards to maintain compliance and accuracy. Specimen validity measures, such as temperature and volume checks, are essential to prevent invalid results and legal vulnerabilities. Selecting HHS-certified labs and integrating specimen validity requirements into collection protocols are crucial for defensible workplace drug testing programs.
Most procurement officers sourcing drug testing supplies focus on price, turnaround time, and panel count. That’s understandable. But understanding drug test cutoffs is where compliance programs actually succeed or fail. A test kit calibrated to the wrong cutoff threshold, or a collection protocol that ignores specimen validity, can invalidate results that would otherwise hold up in federal review, labor disputes, or accreditation audits. This guide breaks down how drug test cutoff levels work, what federal standards require, and what that means for every purchase order you sign.
Regulatory standards and drug test cutoff basics
A drug test cutoff is the minimum analyte concentration in a specimen at which a test reports a positive result. Below that threshold, the test reports negative, regardless of whether trace amounts are present. This design is intentional. It filters out incidental environmental exposure or passive inhalation and focuses on concentrations that indicate actual use.
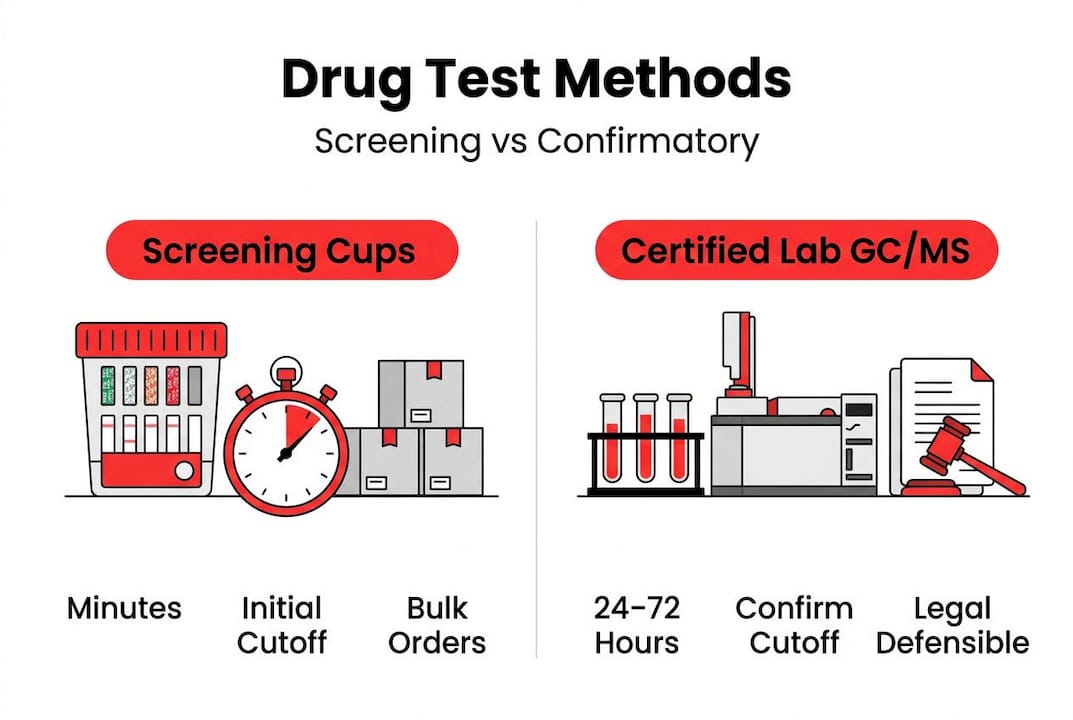
Understanding drug testing thresholds requires knowing there are two distinct tiers in every federally regulated program:
- Initial cutoff (screening): The concentration that triggers a presumptive positive on an immunoassay screen
- Confirmatory cutoff (confirmation): A lower, more specific threshold used by gas chromatography/mass spectrometry (GC/MS) to verify the initial result
The two levels are not the same, and that gap is deliberate. A specimen must first exceed the screening cutoff, then independently meet the confirmatory cutoff under a different analytical method. Both thresholds must be crossed before a result is reported as confirmed positive.
Here’s how the most common federal cutoff values break down:
| Substance | Initial cutoff (ng/mL) | Confirmatory cutoff (ng/mL) |
|---|---|---|
| THC (marijuana metabolites) | 50 | 15 |
| Cocaine metabolites | 150 | 100 |
| Amphetamines | 500 | 250 |
| Opioids (codeine/morphine) | 2,000 | 2,000 |
| Phencyclidine (PCP) | 25 | 25 |
| MDMA | 500 | 250 |
HHS/SAMHSA publishes federal workplace drug testing panels annually with defined initial and confirmatory cutoffs, so these values can and do change. Your procurement contracts should reference the current panel year, not generic “SAMHSA-compliant” language that becomes outdated.
Pro Tip: When evaluating test cup vendors, ask specifically whether their products are calibrated to the current HHS panel year. Many kits on the market still use legacy cutoff values from prior panels, which creates compliance exposure you won’t catch until an audit. Refer to current drug testing standards before locking in any supplier agreement.
Specimen validity requirements and their impact on testing accuracy
Cutoff values only matter if the specimen reaching the lab is legitimate. Specimen validity testing (SVT) exists to catch adulteration, substitution, and dilution before a result is ever calculated. For procurement officers, this means the collection supplies and protocols you specify are part of your compliance chain, not just a logistical detail.
The core specimen validity criteria you need to build into your collection protocols include:
- Volume: A minimum 30 mL of urine is required to perform both initial and confirmatory testing. Split-specimen procedures may require up to 45 mL.
- Temperature: Specimen temperature must fall between 32 and 38 degrees Celsius when measured within four minutes of collection. Outside this range, substitution is suspected.
- Creatinine concentration: Normal range is 2 to 300 mg/dL. Values below 2 mg/dL suggest substitution; values between 2 and 20 mg/dL indicate dilution.
- pH level: Valid specimens fall between pH 4.0 and 9.0. Values outside this range indicate chemical adulteration.
- Oxidizing agents and surfactants: Checked via colorimetric assays to detect common adulterants like bleach, nitrites, or soap.
A specimen that fails validity criteria is reported as rejected for testing, not negative. That distinction is critical. A rejected specimen still triggers consequences under most federal testing programs, including potential “refusal to test” status for the donor. Procurement officers who spec out collection cups without temperature strips or inadequate volume markings are unknowingly creating gaps in their programs.
Pro Tip: When purchasing urine specimen cups in bulk, confirm the cup design includes an integrated temperature strip calibrated to the 32 to 38 degree Celsius range. This single feature prevents the most common and least defensible specimen validity failures during collection.

Certified laboratories and their role in federal drug testing compliance
The chain of compliance does not end with a good collection kit and the right cutoff values. The laboratory processing your specimens must itself be certified under the HHS Mandatory Guidelines. Procurement contracts that specify “accredited lab” without requiring HHS certification specifically are leaving a regulatory gap.
Here is the process a laboratory must complete to earn and maintain HHS certification:
- Submit application to the HHS Substance Abuse and Mental Health Services Administration (SAMHSA)
- Receive and accurately analyze three rounds of performance testing specimens
- Pass an on-site inspection by HHS personnel
- Submit to quarterly proficiency testing to maintain active certification
- Comply with periodic unannounced inspections
HHS-certified labs and Instrumented Initial Testing Facilities (IITFs) must also meet strict chain-of-custody documentation requirements and reporting timelines. This matters in litigation. A confirmed positive result processed by a non-certified lab is legally vulnerable, even if the science was sound.
Key distinctions procurement officers should know:
- Certified labs can perform both initial screening and confirmatory GC/MS testing
- IITFs perform only initial testing and must send presumptive positives to a fully certified lab for confirmation
- Oral fluid testing under federal programs is only available through certified labs, not IITFs
Certified labs maintain status by meeting ongoing performance standards and inspections. The Federal Register publishes an updated list regularly. Before renewing any lab service contract, cross-reference it against the current published list.
Understanding common challenges and nuances in drug test cutoff interpretation
Even a perfectly collected specimen processed by a certified lab can produce a misleading result if the people interpreting the output do not understand how immunoassay screening works. This is where drug test limits explained simply can prevent expensive legal and HR problems.
The most important vulnerabilities in initial screening:
- Cross-reactivity: Immunoassay screens use antibodies that can bind to structurally similar compounds, not just the target drug. Ibuprofen at high doses has triggered false positives for cannabinoids in older assay formats. Certain decongestants can flag amphetamines.
- False negatives from metabolite targeting: Many assays target a specific metabolite rather than the parent drug. If an individual’s metabolism produces atypical metabolite ratios, their result may fall below the cutoff even with documented use.
- Analyte nomenclature inconsistency: When labs use different names for the same analyte across reports, a medical review officer (MRO) or compliance team comparing results across facilities may misread the data.
The federal panel updates address analyte standardization directly, requiring uniform naming conventions across certified labs to reduce exactly this type of misinterpretation. If your current lab reports do not use standardized analyte names, that is a contract compliance issue worth raising immediately.
For procurement, this means the test kits and labs you select should both align with standardized drug screening terminology from the current federal guidelines. A screening product calibrated to an outdated assay format, or a lab that uses non-standard nomenclature, introduces error before the result ever reaches your HR or legal team.
Applying drug test cutoff knowledge to procurement and compliance decisions
Applying all of this to actual purchasing decisions requires a structured evaluation framework. Cutoff values for drug tests, specimen validity, and lab certification cannot be treated as separate procurement checkboxes. They interact.
Use this sequence when evaluating testing supplies and lab partners:
- Confirm cutoff calibration. Verify that test cups and strips are calibrated to the current HHS panel cutoffs for each analyte. Get this in writing from the vendor.
- Check specimen volume capacity. Ensure collection cups support the minimum 30 mL requirement and include volume indicators, particularly for split-specimen programs requiring 45 mL.
- Require temperature strips. Integrated temperature verification is not optional for federally regulated programs.
- Verify lab certification status. Pull the current Federal Register certified lab list before any new contract or renewal.
- Specify IITR or full certification. Define in your contract which certification tier is required based on whether you need confirmatory testing at the same facility.
- Build in panel update reviews. Schedule annual contract reviews timed to HHS panel publication cycles so cutoff values stay current without manual monitoring.
| Feature | Screening test cups | Confirmatory GC/MS (certified lab) |
|---|---|---|
| Speed | Minutes | 24 to 72 hours |
| Cutoff enforcement | Initial cutoffs only | Confirmatory cutoffs applied |
| Legal defensibility | Presumptive only | Fully defensible |
| Cost per test | Lower | Higher |
| Required for federal programs | Yes (initial) | Yes (for positives) |
Pro Tip: Build a side-by-side compliance feature comparison into your RFP template for drug testing contracts. Ask vendors to document cutoff calibration year, specimen volume support, temperature strip inclusion, and lab certification tier in a single response sheet. It removes ambiguity and creates an audit trail. Refer to a solid drug testing program compliance framework before drafting your next RFP.
Why many drug testing programs overlook specimen validity but shouldn’t
Here is the uncomfortable pattern we see repeatedly. Procurement officers invest real effort into selecting the right panel, verifying lab certifications, and documenting cutoff levels. Then a specimen gets rejected because a collector forgot to check the temperature strip within the required four-minute window, or because the collection cup held only 25 mL and the donor was not instructed to provide more.
The result is not a minor inconvenience. A rejected specimen in a federally regulated program can be reported as a refusal to test, which carries the same consequences as a confirmed positive for safety-sensitive positions. All that work on cutoff compliance becomes irrelevant at the collection point.
Specimen validity factors like temperature timing and minimum volume can determine whether results are reported at all, making them just as consequential as the cutoff values everyone focuses on. Yet specimen validity rarely appears as a line item in drug testing RFPs or vendor evaluations.
The fix is not complicated. It requires treating specimen collection supplies and collector training as compliance infrastructure, not just administrative overhead. Collectors need to know the four-minute temperature rule. Collection facilities need to stock the right cups. And procurement officers need to specify these requirements the same way they specify panel coverage or lab certification. Your urine specimen collection protocol is the foundation that everything else is built on. If it has cracks, even the best lab and the most accurate test kit cannot compensate.
Optimizing your drug testing procurement with Buy Test Cup solutions
Buy Test Cup carries drug test cups calibrated to current SAMHSA cutoff standards, with integrated temperature strips, volume indicators, and multi-panel configurations built for compliance-driven programs. Whether you’re running a federal workplace testing program, a healthcare employee screening protocol, or a large-scale corporate compliance initiative, the product catalog covers single-specimen cups, split-specimen kits, oral swabs, and dip strips. Before your next procurement cycle, review the essential drug testing supplies checklist to confirm your current setup covers every validity requirement. And if you’re building or auditing a full program, the drug testing program compliance guide maps the process from collection to reporting in plain language.
Frequently asked questions
What are drug test cutoffs and why do they matter for workplace testing?
Drug test cutoffs are specific analyte concentration thresholds that determine whether a result is reported as positive or negative, ensuring consistent detection standards across labs. HHS/SAMHSA publishes annual cutoff levels for federal workplace drug testing panels to standardize results across all certified facilities.
Why is minimum urine volume important in drug testing?
Minimum volume ensures enough specimen exists for both initial screening and confirmatory testing, preventing results from being voided due to insufficient sample. Protocols require at least 30 mL of urine for initial and confirmatory tests, with split-sample procedures potentially requiring 45 mL.
How does laboratory certification affect drug test procurement decisions?
Only HHS-certified labs can produce results that are legally defensible under federal Mandatory Guidelines, which is non-negotiable for government, DOT, and safety-sensitive programs. Certified labs pass rigorous performance tests and inspections to meet the standards required for federal drug testing programs.
What causes false positive or false negative drug test results?
False positives result from immunoassay cross-reactivity with structurally similar compounds, while false negatives occur when drug concentrations fall below the assay’s detection threshold or targeted metabolites are absent. Immunoassays are vulnerable to cross-reactivity, and detection limits directly affect how accurately low-level presence is captured.
How can procurement officers ensure compliance with federal drug testing standards?
Select test supplies calibrated to current SAMHSA cutoff values, require HHS-certified labs in all contracts, and build specimen validity protocols into collection procedures from the start. Strict adherence to panel cutoffs and certified labs is the baseline for a legally defensible, audit-ready testing program.